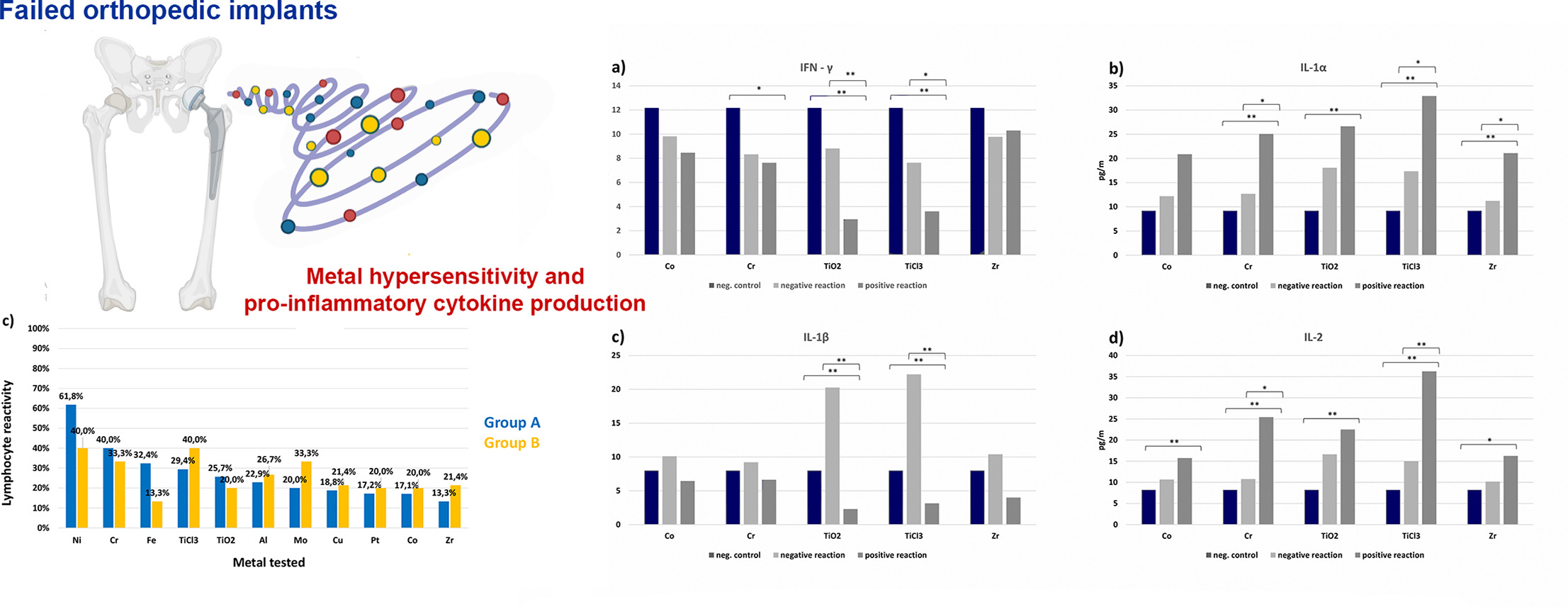
• In 40% of patients, implant failure is due to hypersensitivity to the contained metal
• In failed orthopedic implants the most frequent metals are Ni, Cr, Ti, Fe and Mo
• Patients with Ti hypersensitivity after Ti stimulation showed major changes in pro-inflammatory cytokine production
• Patients with titanium hypersensitivity may lead to titanium implant failure
• Metal hypersensitivity tests should be performed on patients prior to surgery
Abstract
Orthopedic implants heal well without complications in most patients but fail for unclear reasons in some individuals. This study determined the relevance of metal hypersensitivity in patients with failed orthopedic implants and those requiring orthopedic implant surgery. The study included 35 patients with failed orthopedic implants and 15 subjects scheduled for orthopedic implant surgery. The production of selected pro-inflammatory cytokines was measured in patients with failed orthopedic implants. Metal hypersensitivity was measured in all subjects using the MELISA® test. Of common metals in orthopedic alloys, the patients with failed orthopedic implants responded most frequently to nickel, chromium, titanium, iron, and molybdenum. Hypersensitivity to metals found in implants was measured in 40% of patients with failed implants. The study also showed that titanium exposure in patients with titanium hypersensitivity might lead to implant failure. Metal hypersensitivity testing should be offered to patients before surgery to minimize the risk of implant failure.
1. Introduction
A continually increasing demand for orthopedic implants results in a growing requirement for orthopedic materials with excellent mechanical properties, durability, and biocompatibility.
Orthopedic implants are commonly made of cobalt-chromium alloys, stainless steel, titanium alloys, and zirconia. These implants heal well in most patients; nevertheless, orthopedic implants fail in some [1]. When infection and instability have been excluded, metal hypersensitivity should be considered as a cause of primary implant failure [[2], [3], [4], [5]].
The pathogenesis of total joint replacement failure is multifactorial. Corrosion and wear of implants result in metal ion release, which may then lead to sensitization and even implant failure, owing to acquired immune reactivity [6]. There are two predominant tissue responses to periprosthetic metal wear debris: a nonspecific macrophage-mediated granulomatous response and a lymphocyte-dominated response mediated by T cells, some of which have immunological memory. Delayed-type hypersensitivity responses may accelerate the aseptic loosening of arthroplasty implants [7,8]. Metal hypersensitivity generally leads to pain and swelling, as well as cutaneous symptoms [[9], [10], [11]]. In addition to these well-known symptoms, an extensive number of more unusual systemic symptoms, connected to metal hypersensitivity, have been described in the literature [12]. Metal hypersensitivity diagnosis should be performed in patients with painful joint arthroplasty when other possible causes have been ruled out [13]. To determine delayed-type hypersensitivity responses, patch or lymphocyte transformation tests (LTTs) can be used. Patch testing is a procedure used to determine whether a specific substance causes allergic inflammation of a patient's skin. It is intended to produce a local allergic reaction on the skin, where the diluted allergens are placed [14]. The limitations of patch testing include the possibility of hapten exposure inducing sensitization, lack of reproducibility, variations in preparations, time of reading, as well as the visual perception of skin reactions which can vary depending on the physician's experience and training [15,16]. Implant-related type IV hypersensitivity reactions are mediated by sensitized T cells and the relationship between skin hypersensitivity and systemic hypersensitivity is ill-defined [[17], [18], [19]]. LTTs are better suited for measuring delayed-type IV hypersensitivity reactions than patch testing [20]; therefore, in this study, the MELISA® test was used. It is a validated and optimized LTT based on measuring the proliferation of peripheral blood lymphocytes in vitro after incubation with metal salts [[21], [22], [23]].
Metal ions released as wear debris from orthopedic implants bind to serum proteins and form hapten-like complexes that can be identified by the immune system as antigens and may activate the immune system [[24], [25], [26]].
Important factors in immune reactivity include cytokines; water-soluble substances with biological effects produced by different types of immuno-competent cells, through which the cells influence each other. Metals present in orthopedic implants, such as chromium, cobalt, titanium, and zirconium, may cause an increase in the production of pro-inflammatory cytokines and thus activation of antigen-presenting cells and/or neoantigen induction; as a result the immune reaction of Th0 lymphocytes activation and differentiation to Th1 or Th2 lymphocyte clones develops [27]. Metals participate in antibacterial immune reactions through macrophage activation and may take part in an inflammatory reaction via delayed-type hypersensitivity. Pro-inflammatory cytokines, including IFN-γ, IL-1, IL-2, IL-6, IL-17, and TNF-α, are predominantly derived from the innate immune cells and Th1 lymphocytes. Anti-inflammatory cytokines, including IL-4, IL-5, IL-10, and IL-13, are synthesized from Th2 lymphocytes. Cytokines can be determined by multiplex analysis Luminex, one of the most recently developed immuno-analytical methods.
Current materials research is focused on increasing the biocompatibility of materials used in medical implants, for example by modifying alloys to increase corrosion resistance or by application of surface coating. Research on new functional carbon-based coatings shows both increased long-term durability and increased corrosion resistance [[28], [29], [30]]. Carbon coating was used successfully in a young boy with syndromic scoliosis who had metal rods implanted and developed severe post-operative symptoms. MELISA® testing showed that the boy was hypersensitive to several metals found in his implant. Symptoms resolved after the rods were removed. Eventually the rods were “camouflaged” from the patient's immune system by an innovative carbon coating and the boy was able to tolerate the implant [31].
However, the risk of implant failure must be minimized and, ideally avoided, in advance. This study aimed to determine metal hypersensitivity in subjects who required orthopedic implant surgery and in patients with failed orthopedic implants, as well as monitor the production of selected pro-inflammatory cytokines in patients with failed orthopedic implants.
2. Methods
This study is designed as a case-control study with Level III Evidence.
2.1. Examined groups
Based on informed consent forms and in accordance with the Helsinki declaration, a group of 50 subjects; 14 men and 36 women, with the mean age of 60.2 years, were examined.
In total, 35 patients with failed total hip or knee endoprosthesis (32 patients) or with another failed type of implant surgery (3 patients) constituted patient Group A. Fifteen subjects with planned implantation of a total hip or knee endoprosthesis constituted a control Group B.
Group A consisted of the following: 21 patients with knee replacements, 10 patients with hip replacements, one patient with total knee and hip replacements, two patients with titanium spinal fixation implants, and one patient with a titanium shoulder replacement. The alloys in the implants used were mostly titanium-based (present in 20 of the knee implants, nine of the hip replacements, in both spinal implants, once in the titanium shoulder implant). Implants made up of cobalt-chromium alloys were present in fewer cases (twice in total knee implants, twice in total hip replacements).
In all the patients from Group A, the referring orthopedic surgeons excluded mechanical complications or infections as possible causes of implant failure. Patients were referred for examination at our institute by orthopedic surgeons for suspected hypersensitivity to the implanted material. The reasons for the referral were: intense pain in 17 patients, intense pain associated with swelling in 10 patients, swelling in 5 patients, and rash in 3 patients. All patients from Group A stated that during the pre-surgery examination, they were not tested for metal hypersensitivity by patch test or MELISA® testing. Additionally, they had no clinical symptoms of metal hypersensitivity before the endoprosthesis surgery.
In Group B, seven patients were examined before total knee arthroplasty, seven patients were examined before total hip arthroplasty, and one patient was examined before total knee and hip arthroplasty. All patients from Group B stated during the examination that they were patch test positive to chromium and/or cobalt and/or nickel and/or they had clinical symptoms of metal hypersensitivity in the past. Given their clinical histories, MELISA® testing was performed before endoprosthesis surgery.
2.2. Clinical examination
For all the study subjects, a detailed personal and family history was taken, focused on their metal exposure. For these purposes, target-compiled questionnaires were used.
2.3. MELISA® test
The MELISA® test is based on evaluating the proliferation of peripheral blood memory cells in vitro after incubation with metal salts [21,22]. Ten milliliters of peripheral venous blood were collected and centrifuged to provide the patients' autologous serum. Heat-inactivated autologous serum was used for the cultivation of lymphocytes. 30 ml of peripheral venous blood was collected and mixed with an equal amount of RPMI 1640 medium containing 10 mM HEPES, gentamycin, and glutamine. The blood was layered on a Ficoll-Paque gradient (Histopaque, Sigma Aldrich) and centrifuged at 600 g for 30 min. Mononuclear cells were collected from the interface, washed twice, then mixed with 5 ml of RPMI 1640 medium containing 20% of inactivated autologous serum. Plastic-adherent cells were partially depleted from leukocyte suspension by incubation on plastic surfaces for 40 min at 37 °C. After incubation, the lymphocytes were counted and diluted with RPMI 1640 enriched with 10% autologous serum and glutamine into a final dilution of 1 × 106 cells/ml. Lymphocytes were cultivated for five days with metal salts solutions in an atmosphere of 5% CO2 in humidified air at 37 °C. All patients in this study were tested to nickel, chromium, iron, titanium (in the form of chloride and oxide), aluminum, molybdenum, copper, platinum, cobalt and zirconium. Details of the specific metal salts and their concentrations are described by Stejskal et al. [21]. Control cultures were incubated under the same conditions in the absence of metal salt solutions. As a positive control, lymphocytes were cultivated with Pokeweed mitogen (10 μg per ml, Sigma, USA). After five days' cultivation, lymphocyte cultures were split into two parts. One part was used to measure lymphocyte proliferation by 3H thymidine incorporation (Perkin Elmer, USA), as described in the article by Stejskal et al. [21]. The second part was frozen at −20 °C to determine pro-inflammatory cytokine production.
The rate of lymphocyte proliferation in metal-treated cultures was compared to the rate in non-stimulated cultures and evaluated by a Stimulation index (SI): counts per minute in metal-treated cultures divided by counts per minute in non-treated cultures.
An SI of less than two was regarded as a negative reaction, SI 2.01–3 as a weakly positive reaction, SI 3.01–10 as a positive reaction, and SI higher than ten was regarded as a strongly positive reaction [20].
2.4. Pro-inflammatory cytokine production in lymphocyte cultures
Frozen lymphocyte cultures were thawed to determine pro-inflammatory cytokine production.
The establishment of pro-inflammatory cytokines IFN-γ, IL-1α, IL-1β, IL-2, IL-6, IL-17, and TNF-α production was performed in supernatants of lymphocyte tissue cultures after cultivation with metal antigens of cobalt dichloride (CoCl2 · 6H2O, Sigma Aldrich, USA), chromium trichloride (CrCl3 · 6H2O, Sigma Aldrich, USA), titanium dioxide (TiO2, Sigma Aldrich, USA), titanium trichloride (TiCl3, Sigma Aldrich, USA), zirconium dioxide (ZrO2, Sigma Aldrich, USA) and in non-stimulated negative control cultures of lymphocytes by multiplex analysis using standard Luminex® Performance Assay kits (RnDSystems, USA). The test was performed according to the instructions for use provided with this commercial kit.
Before taking measurements, a protocol was created by programming the Luminex 100 IS software. The protocol included information about the standard, number of measured cytokines, regions of individual cytokines detection, and their concentration. The measurement of each well in the plate lasted for a maximum of 94 s. During that time, labeled microparticles with bonded cytokines were harvested and analyzed.
2.5. Statistics
The collected data were statistically processed using MS Excel 2016 and the Data analysis tool pack add-in statistical software, language R (Rstudio). For calculations, descriptive statistics were used - mean and standard deviation. The normal distribution of the samples was tested by the Shapiro-Wilk test. For hypothesis testing, an F-test for equality of variances and a two-tailed two-sample Student's t-test to test the equality of mean values were used. Hypothesis testing was performed at a significance level of 0.01 and 0.05.
3. Results
3.1. Metal hypersensitivity testing
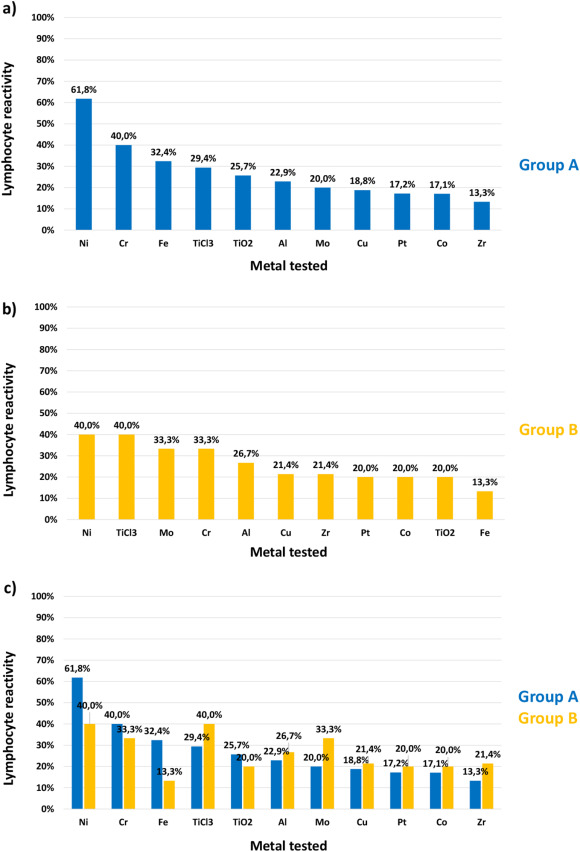
Results of the lymphocyte reactivity to different metal salts in patients with a hypersensitivity to tested metals (Group A), in controls (Group B), and the comparison are presented in Fig. 1.
Fig. 1
Results of the lymphocyte reactivity to different metal ions in Group A (patients with failed implant surgery) are presented in Fig. 1a.
Reactivity was most frequent to nickel (61.8%), followed by chromium (40%), iron (32.4%), titanium (in the form of chloride) (29.4%), titanium (in the form of oxide) (25.7%), aluminum (22.9%), molybdenum (20%), copper (18.8%), platinum (17.2%), cobalt (17.1%) and zirconium (13.3%).
Results of the lymphocyte reactivity to metal salts in Group B controls are presented in Fig. 1b and are in the order: nickel and titanium (in the form of chloride) (40%), molybdenum and chromium (33.3%), aluminum (26.7%), copper and zirconium (21.4%), platinum, cobalt and titanium (in the form of oxide) (20%) and iron (13.3%), respectively.
Patients in the two groups were not matched for gender due to a limited number of patients. We compared sensitivity to metals between women and men. We found that women reacted more than men to platinum (+25%) and copper (+15.2%). Men reacted more than women to titanium dioxide (+16.3%) and nickel (+13%). The differences in reactivity to other metals tested were <10%.
Comparing the reactivity to metal salts with the composition of failed orthopedic implants used in the patients of Group A, titanium hypersensitivity to at least one of the tested titanium salts was identified in 12 out of the 31 patients with a titanium-based implant, i.e., in 38.7%. Out of 4 patients with implants based on cobalt-chromium alloys, a hypersensitivity to at least one of these metals was identified in two patients, i.e., in 50%.
Fourteen out of the 35 patients in Group A, i.e., 40% of patients, demonstrated hypersensitivity to the material that is the basis of the failed implant.
3.2. Cytokine production
We examined a total of 168 samples of lymphocyte cultures from 28 randomly selected patients, in which the simultaneous determination of the concentration of 7 pro-inflammatory cytokines - IFN-γ, IL-1α, IL-1β, IL-2, IL-6, IL-17, and TNF-α - in lymphocyte cultures without stimulation, and in lymphocyte cultures after stimulation with chromium, cobalt, titanium in the form of oxide, titanium in the form of chloride and zirconium were performed.
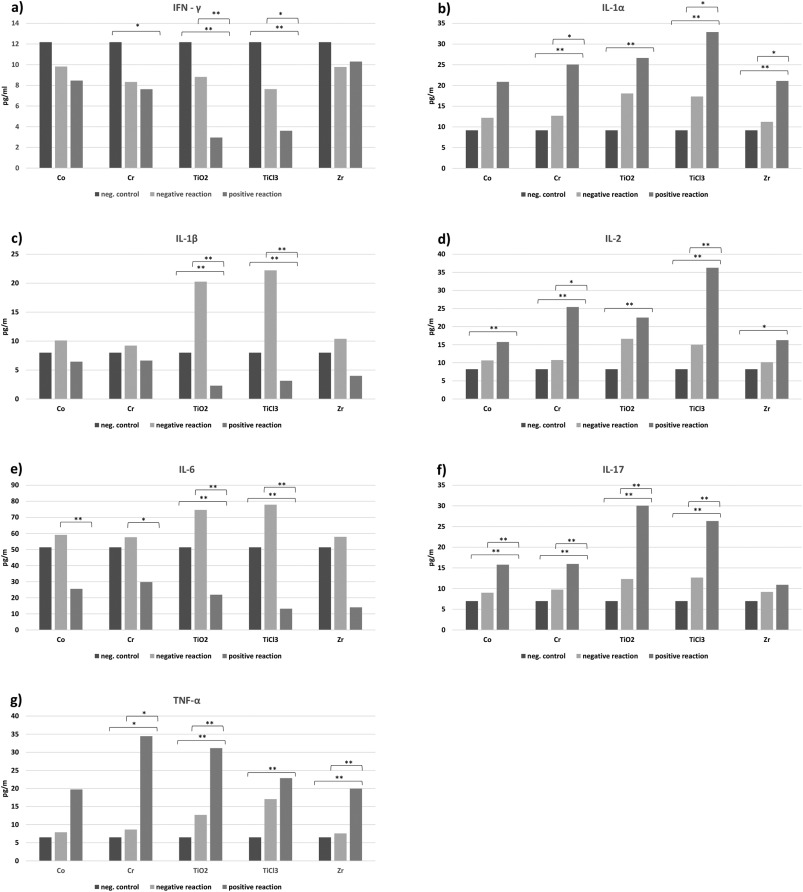
In Fig. 2, results of cytokines IFN-γ, IL-1α, IL-1β, IL-2, IL-6, IL-17 and TNF-α production in lymphocyte cultures without stimulation (negative control), in lymphocyte cultures from patients without diagnosed hypersensitivity (negative reaction) and in lymphocyte cultures from patients with diagnosed hypersensitivity (positive reaction) are shown.
Fig. 2
Results of IFN-γ production (Fig. 2a) show a decrease after stimulation by all tested metal antigens. This decrease was more significant in cultures from patients with diagnosed metal hypersensitivity (positive reaction). The highest decrease (statistically significant) was found in cultures from patients with diagnosed hypersensitivity to titanium (positive reaction) stimulated by titanium antigens, and the lowest decrease (not statistically significant) was found in cultures stimulated by zirconium and cobalt antigens.
An increase in IL-1α production after stimulation by all tested metal antigens was observed (Fig. 2b). The highest increase was found in cultures from patients with diagnosed hypersensitivity to titanium (positive reaction) stimulated by titanium antigens, and the lowest increase was found in cultures from patients without diagnosed hypersensitivity (negative reaction) stimulated by cobalt and zirconium antigens. Results of IL-1β production (Fig. 2c) show an increase after stimulation by all tested metal antigens in cultures from patients without diagnosed hypersensitivity (negative reaction) and a decrease in IL-1β production after stimulation by all tested metal antigens in cultures from patients with diagnosed hypersensitivity (positive reaction). The highest increase was found in cultures from patients without diagnosed hypersensitivity to titanium (negative reaction) stimulated by titanium antigens, and the highest decrease was found in cultures from patients with diagnosed hypersensitivity to titanium (positive reaction) stimulated by titanium antigens. Results of IL-2 production (Fig. 2d) show an increase after stimulation by all tested metal antigens. The highest increase was found in cultures from patients with diagnosed hypersensitivity to titanium and chromium (positive reaction) stimulated by titanium and chromium antigens, and the lowest increase was found in cultures from patients without diagnosed hypersensitivity to cobalt, chromium, and zirconium (negative reaction) stimulated by cobalt, chromium and zirconium antigens. Results of IL-6 production (Fig. 2e) show an increase after stimulation by all tested metal antigens in cultures from patients without diagnosed hypersensitivity (negative reaction) and a decrease in IL-6 production after stimulation by all tested metal antigens in cultures from patients with diagnosed hypersensitivity (positive reaction). The highest increase was found in cultures from patients without diagnosed hypersensitivity to titanium (negative reaction) stimulated by titanium antigens, and the highest decrease was found in cultures from patients with diagnosed hypersensitivity to titanium (TiCl3) and zirconium (positive reaction) stimulated by titanium (TiCl3) and zirconium antigens. Results of IL-17 production (Fig. 2f) show an increase after stimulation by all tested metal antigens. The highest increase was found in cultures from patients with diagnosed hypersensitivity to titanium (positive reaction) stimulated by titanium antigens, and the lowest increase was found in cultures from patients without diagnosed hypersensitivity to cobalt, chromium, and zirconium (negative reaction) stimulated by cobalt, chromium and zirconium antigens.
Last, an increase in TNF-α production after stimulation by all tested metal antigens was observed (Fig. 2g). The highest increase was found in cultures from patients with diagnosed hypersensitivity to chromium and titanium (TiO2) (positive reaction) stimulated by chromium and titanium (TiO2) antigens, and the lowest increase was found in cultures from patients without diagnosed hypersensitivity to cobalt, chromium, and zirconium (negative reaction) stimulated by cobalt, chromium and zirconium antigens.
4. Discussion
Several metals, either alone or as part of an alloy, are incorporated in the design of medical implants. Commonly present metals in implants are elements essential for the human body, playing a specific and fundamental role in human metabolism (copper, iron, cobalt and possibly nickel). Other metallic elements used in implants, on the other hand, are not essential for humans (titanium and aluminum) [32]. Both essential and non-essential metals, when present at sufficiently high concentrations, can disrupt normal biological functions and cause toxicity [33]. Metal toxicity as well as metal hypersensitivity can affect various tissues including the kidney, liver, heart, immune and nervous systems. According to this study, in patients with failed total hip or knee endoprosthesis, the most frequently found hypersensitivity was to nickel. This result is consistent with the literature reporting that nickel is the most common metal allergen. Most patients referred to this study had titanium-based orthopedic implants (31 cases), and the minority had cobalt‑chromium alloys (4 cases). Therefore, monitoring immune reactions to metals commonly used in orthopedic alloys - mainly titanium, chromium, cobalt as well as molybdenum and nickel, appears to be significant to ensure the success of orthopedic surgery. Zirconium can also be tested, as zirconia appears to be a suitable alternative in those with metal hypersensitivity. In this study, 40% of patients with failed total hip or knee endoprosthesis had a hypersensitivity to chromium, 29% to titanium chloride, 26% to titanium oxide, and 17% to cobalt. When correlating metal reactivity with the composition of failed orthopedic implants, results were as follows: hypersensitivity to titanium was found in 39% of patients with failed titanium-based implants, and hypersensitivity to chromium and/or cobalt in 50% of patients with implants based on cobalt‑chromium alloys. Overall, hypersensitivity to failed implant composition was determined in 40% of patients with failed implants.
To minimize the risk of implant failure, metal hypersensitivity testing should be offered to patients (especially those with autoimmune diseases, asthma, and/or allergies) before surgery. In those where metal hypersensitivity is suspected or confirmed, metal-free implants should be used. Such implants are made of zirconia ceramics and ultra-high-molecular-weight-polyethylene, very stable and biocompatible compounds. Nevertheless, zirconia may very rarely cause allergic reaction [34] and reaction to zirconium should be measured by the MELISA®. Nevertheless, a 4-year-follow-up study on 38 metal-allergic patients with zirconia ceramic knee replacement system showed excellent immuno-allergological compatibility, offering a safe option for patients with prior hypersensitivity reactions to metallic materials [35]. Ultra-high-molecular-weight-polyethylene may degrade through wear and particulate wear debris may cause local osteolysis [36]. If this happens, it is possible to exchange the isolated liner with the use of an acetabular cup that yielded 98.8% acetabular survival for aseptic loosening at up to 15 years [37].
The effect of metals on cytokine production has already been proven in the past [38,39]. In this study, pro-inflammatory cytokine production was monitored, as cytokines represent a specific type of immune reaction and play a crucial role in pro-inflammatory reactions. A decrease in IFN-γ production after stimulation by all tested metal antigens was found. The most significant decreases were found in cultures from patients with diagnosed hypersensitivity to titanium stimulated by titanium, and the least significant decrease in cultures stimulated by zirconium. These results are in concordance with previously published results of IFN-γ production by lymphocyte cultures of patients with failed dental titanium implants [39]. Increases in IL-1α, IL-2, IL-17, and TNF-α production after stimulation by all tested metal antigens with the most significant increase in cultures from patients diagnosed with hypersensitivity to titanium stimulated by titanium (in TNF-α production also in cultures from patients with diagnosed hypersensitivity to chromium stimulated by chromium) were determined. The least significant increase was found in cultures from patients without diagnosed hypersensitivity to zirconium stimulated by zirconium. An increase in IL-1β and IL-6 production was found after stimulation by all tested metals in cultures from patients without diagnosed hypersensitivity to the corresponding metal, and a decrease in IL-1β and IL-6 production after stimulation by metals tested in cultures from patients with diagnosed hypersensitivity to the corresponding metal. The most significant changes were found in cultures from patients with diagnosed hypersensitivity to titanium stimulated by titanium. These results are in concordance with previously published results of IL-1β and IL-6 production in lymphocyte cultures from patients with failed dental titanium implants where increased levels of IL-1β and IL-6 production were found in patients with well-integrated implants compared to patients with failed implants [39,40].
Langton et al. [41] carried out an investigation to identify HLA alleles associated with development of delayed-type hypersensitivity following metal-on-metal cobalt-chromium hip arthroplasty. The dominant, significant positive association with implant failure was seen with DQA1*02:01, DQB1*02:02, and DRB1*07:01. A protective effect was seen with the alleles DQA1*01:01, DQB1*05:01, and DRB1*01:01. Class I HLA allele distributions did not differ between the groups of patients with and without implant failure. Determination of specific genotypes significantly associated with greater risk of delayed-type hypersensitivity-related prosthetic failure may improve implant selection if there will be more studies clarifying if this association is valid also for other metallic materials used as orthopedic prostheses and if a special assay to identify patients at risk will be developed. Nevertheless, such assay could not identify the most appropriate implant material for an individual patient. Our findings in this study confirmed that the MELISA® test can identify the most suitable implant material for patients with hypersensitivity to metals.
Some limitations of this study should be reported. Firstly, the small sample size, which was due to a limited period, as this was a three-year study. Secondly, patients with failed implants due to mechanical complications or infections were excluded. Further, bone cements were not tested, and there was no gender matching done in the groups (due to the limited source of defined patients and limited time). Whether implant failure occurred due to pre-existing metal hypersensitivity or if metal hypersensitivity resulted from secondary sensitization to metal debris released from failing implants remain questions that need to be clarified.
The MELISA® test has many advantages compared to patch testing, yet possible limitations of the MELISA® test should also be pointed out. For testing a relatively large volume of blood is required, which must reach a laboratory licensed to perform testing within 48 h to ensure viability of the cells. Results may take over a week to obtain, and the test method is labour intensive, meaning testing can be expensive for patients if not covered by healthcare insurance.
5. Conclusions
In this study, 40% of patients with failing implants had hypersensitivity reactions to a metal present in their implant, as measured by the MELISA® test. In these patients, the production of pro-inflammatory cytokines was influenced the most by titanium stimulation in patients with diagnosed titanium hypersensitivity. Titanium exposure in patients with titanium hypersensitivity may lead to titanium implant failure. To minimize the risk of implant failure, metal hypersensitivity testing should be offered to patients (especially those with autoimmune diseases, asthma, and/or allergies) before surgery. This would enable the most appropriate implant material to be selected.
Utilizamos cookies para oferecer melhor experiência, melhorar o desempenho, analisar como você interage em nosso site e personalizar conteúdo.
Aceitar CookiesSaiba Mais